Background: Infection with the Human Immunodeficiency Virus (HIV) is responsible for the terminal stage of Acquired Immunodeficiency Syndrome (AIDS), which was a latent infection until the introduction of antiretroviral treatment. The progression to chronicity of this infection leads to chronic inflammation that facilitates the occurrence of opportunistic infections such as herpes simplex virus types 1 and 2 (Herpes Simplex Virus-1 (HSV-1) and Herpes Simplex Virus-2 (HSV-2)). The lack of data on these viruses has led to the present study. Objective: aimed to determine the seroprevalence of IgG antibodies against herpes simplex virus types 1 and 2 in children born HIV-positive to HIV-positive mothers with an undetectable viral load and receiving antiretroviral treatment at the Yaoundé University Teaching Hospital (YUTH). Method: The study was cross-sectional conducted after 12 months of follow up. After administering a questionnaire, a blood sample was obtained from each participant in an EDTA tube and analyzed using rapid diagnostic tests for the detection of specific IgM/IgG antibodies. Statistical analysis was performed using Microsoft Excel 2019 and SPSS version 25. A P-value <0.05 was considered statistically significant at a 95% confidence interval. Result: Among the 74 participants, 51 were female, resulting in a sex ratio of 0.45. In the population of children born HIV-positive, the seroprevalence was 93.24% (n=69) for IgG anti-HSV-1, 93.24% (n=69) for IgG anti-HSV-2, and 93.24% (n=69) for IgG anti-HSV-1/-2. The seroprevalence of IgM anti-HSV was found to be zero; however, the prevalence of IgG anti-HSV was 93.24%. The seroprevalence of HSV-1/-2 was associated with the age of the participants. Conclusion: It can be concluded that the herpes simplex virus circulates in Cameroon, with a high presence of anti-HSV-1/-2 antibodies in the population born HIV-positive to HIV-positive mothers. It becomes important to implement systematic diagnostic measures for children born HIV-positive to HIV-positive mothers, and its transmission is associated with various risk factors.
| Published in | International Journal of Biomedical Engineering and Clinical Science (Volume 11, Issue 3) |
| DOI | 10.11648/j.ijbecs.20251103.11 |
| Page(s) | 40-46 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
YUTH, HSV-1, HSV-2, HIV, AIDS
Type of HSV | Size (n=74) | IC95 | Percentage (%) |
|---|---|---|---|
HSV-1 | 69 | [84.93-97.77] | 93.24 |
HSV-2 | 69 | [84.93-97.77] | 93.24 |
HSV-1/-2 | 69 | [84.93-97.77] | 93.24 |
Absence of HSV-1/-2 | 5 | [2.23-15.07] | 6.76 |
74 (100%) | |||
Number | Gender | HSV-1 only | HSV-2 only | HSV-1+HSV-2 | Absence of HSV-1/-2 | |
|---|---|---|---|---|---|---|
HIV infected persons | ||||||
1 | Male sex (n=23/74, 31.1%) | N | 21 | 21 | 21 | 2 |
% | 91.30 | 91.30 | 91.30 | 8.7 | ||
2 | Female sex (n=51/74, 68.92) | N | 48 | 48 | 48 | 3 |
% | 94.12 | 94.12 | 94.12 | 5.9 | ||
Age group (years) | n (%) | Alcohol consumption n (%) | HSV-1/-2 | Tobacco intake n (%) |
|---|---|---|---|---|
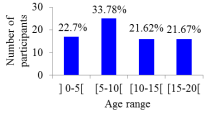
[0-5] | 17 (22.97) | 0 | 17 (24.64) | 0 |
[5-10] | 25 (33.78) | 0 | 21 (30.43) | 0 |
[10-15] | 16 (21.62) | 3 (4.05) | 16 (23.19) | 9 (12.16) |
[15-20] | 16 (21.62) | 14 (18.91) | 15 (21,74) | 9 (12.16) |
Total 74 (100%) | ||||
Groups of CD4+ LT count (cellules/mm3) | HSV-1 n(%) | HSV-2 n(%) | HSV-1/-2 n(%) | Size (%) | P-Value |
|---|---|---|---|---|---|
[500-1600] | 41 (91.11) | 41 (91.11) | 41 (91.11) | 45 (60.8) | 0.002 |
[350-499] | 2 (2.7) | 2 (2.7) | 2 (2.7) | 2 (2.7) | 0.05 |
[200-349] | 23 (95.83) | 23 (95.83) | 23 (95.83) | 24 (32.4) | 0.002 |
[0-200] | 3 (4.05) | 3 (4.35) | 3 (4.35) | 3 (4.1) | 0.05 |
AIDS | Acquired Immunodeficiency Syndrome |
HIV | Human Immunodeficiency Virus |
HSV-1 | Herpes Simplex Virus Type 1 |
HSV-2 | Herpès Simplex Virus Type 2 |
HSV | Herpes Simplex Virus |
PLHIV | People Living with HIV |
YUTH | Yaoundé University Teaching Hospital |
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [2] | Campos-Arjona R, García-Pinilla JM, de Teresa-Galván E. Acute heart failure. Med. 2019; 12(89): 5237-44. |
| [3] | Ural D, Çavuşoğlu Y, Eren M, Karaüzüm K, Temizhan A, Yılmaz MB, et al. Akut kalp yetersizliği tanı ve tedavisi. Anatol J Cardiol. 2015; 15(11): 860-89. |
| [4] | Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Vol. 145, Circulation. 2022. 895-1032 p. |
| [5] | Gallagher J, McDonald K, Ledwidge M, Watson CJ. Heart Failure in Sub-Saharan Africa. Card Fail Rev. 2018; 4(1): 1. |
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
| [7] | Gtif I, Bouzid F, Charfeddine S, Abid L, Kharrat N. Heart failure disease: An African perspective. Arch Cardiovasc Dis. 2021; 114(10): 680-90. |
| [8] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from: |
| [9] | S. Ogah O, Adebiyi A, Sliwa K. Heart Failure in Sub-Saharan Africa. Top Hear Fail Manag. 2019. |
| [10] | Olatayo Adeoti A, Adekunle Ajayi E, Oladimeji Ajayi A, Ayokunle Dada S, Olusesan Fadare J, Akolawole M, et al. Pattern and Outcome of Medical Admissions in Ekiti State University Teaching Hospital, Ado-Ekiti-A 5 Year Review. Am J Med Med Sci. 2015; 2015(2): 92-8. Available from: |
| [11] | Elyamani R, Soulaymani A, Hami H. Epidemiology of Cardiovascular Diseases in Morocco: A Systematic Review. Rev Diabet Stud. 2021; 17(2): 57-67. |
| [12] | Ogah OS, Stewart S, Falase AO, Akinyemi JO, Adegbite GD, Alabi AA, et al. Contemporary profile of acute heart failure in Southern Nigeria: Data from the abeokuta heart failure clinical registry. JACC Hear Fail. 2014; 2(3): 250-9. |
| [13] | Makubi A, Hage C, Lwakatare J, Kisenge P, Makani J, Rydén L, et al. Contemporary aetiology, clinical characteristics and prognosis of adults with heart failure observed in a tertiary hospital in Tanzania: The prospective Tanzania Heart Failure (TaHeF) study. Heart. 2014; 100(16): 1235-41. |
| [14] | Okello S, Rogers O, Byamugisha A, Rwebembera J, Buda AJ. Characteristics of acute heart failure hospitalizations in a general medical ward in Southwestern Uganda. Int J Cardiol. 2014; 176(3): 1233-4. Available from: |
| [15] | Tirfe M, Nedi T, Mekonnen D, Berha AB. Treatment outcome and its predictors among patients of acute heart failure at a tertiary care hospital in Ethiopia: a prospective observational study. BMC Cardiovasc Disord. 2020; 20(1): 16. Available from: |
| [16] | Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10. |
| [17] | Mwita JC, Dewhurst MJ, Magafu MGMD, Goepamang M, Omech B, Majuta KL, et al. Presentation and mortality of patients hospitalised with acute heart failure in Botswana. Cardiovasc J Afr. 2017; 28(2): 112-7. |
| [18] | Carlson S, Duber HC, Achan J, Ikilezi G, Mokdad AH, Stergachis A, et al. Capacity for diagnosis and treatment of heart failure in sub-Saharan Africa. Heart. 2017; 103(23): 1874-9. |
| [19] | Talle MA, Bonny A, Scholtz W, Chin A, Nel G, Karaye KM, et al. Status of cardiac arrhythmia services in Africa in 2018: A PAsCAr sudden Cardiac death task Force report. Cardiovasc J Afr. 2018; 29(2): 115-21. |
| [20] | Bukhman AK, Nsengimana VJP, Lipsitz MC, Henwood PC, Tefera E, Rouhani SA, et al. Diagnosis and Management of Acute Heart Failure in Sub-Saharan Africa. Curr Cardiol Rep. 2019; 21(10). |
| [21] | Fourcade L, Massoure PL, Roche NC, Lamblin G, Topin F, Dehan C. la perspective d ’ une transition épidémiologique Heart failure patterns in Djibouti : epidemiologic transition. 2013; 211-6. |
| [22] | Boombhi J, Moampea M, Kuate L, Menanga A, Hamadou B, Kingue S. Clinical Pattern and Outcome of Acute Heart Failure at the Yaounde Central Hospital. OALib. 2017; 04(03): 1-8. |
| [23] | Tigabe M, Fentahun A, Getawa S, Gelaye KA, Gebreyohannes EA. Clinical Characteristics and In-Hospital Outcome of Acute Heart Failure Patients Admitted to the Medical Ward of University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. Vasc Health Risk Manag. 2021; 17: 581-90. Available from: |
| [24] | James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392(10159): 1789-858. |
| [25] | Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure Measuring an epidemic. 2020; 7-9. |
| [26] | Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005; 149(2): 209-16. |
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [28] | Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017; 19(10): 1242-54. |
| [29] | Follath F, Yilmaz MB, Delgado JF, Parissis JT, Porcher R, Gayat E, et al. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011; 37(4): 619-26. |
| [30] | Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr Heart Fail Rep. 2017; 14(5): 385-92. |
| [31] | Bocchi EA. Heart Failure in South America. 2013; 147-56. |
| [32] | Rockstroh K, Thienemann F, Sliwa K. Clinical update HIV and the heart : the impact of antiretroviral therapy : a global perspective. 2013; 3538-46. |
| [33] | Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: Epidemiological profile and challenges. Nat Rev Cardiol. 2017; 14(5): 273-93. |
| [34] | Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018; 391(10120): 572-80. Available from: |
| [35] | Baldi I, Azzolina D, Berchialla P, Gregori D, Corrao G. Comorbidity-adjusted relative survival in newly hospitalized heart failure patients: a population-based study. Int J Cardiol. 2017; Available from: |
| [36] | Deursen VM Van, Urso R, Laroche C, Damman K, Dahlström U, Tavazzi L, et al. Co-morbidities in patients with heart failure : an analysis of the European Heart Failure Pilot Survey. |
| [37] | Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur Heart J. 2006; 27(22): 2725-36. |
| [38] | Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, et al. Clinical Features and Outcome in Hospitalized Heart Failure in Japan (From the ATTEND Registry). 2013; 77(April): 944-51. |
| [39] | de Albuquerque DC, Neto JD de S, Bacal F, Rohde LEP, Bernardez-Pereira S, Berwanger O, et al. I Brazilian registry of heart failure - Clinical aspects, care quality and hospitalization outcomes. Arq Bras Cardiol. 2015; 104(6): 433-42. |
| [40] | Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Clinical characteristics & outcome of acute heart failure in Korea: Results from the Korean acute heart failure registry (KorAHF). Korean Circ J. 2017; 47(3): 341-53. |
| [41] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Articles Global mortality variations in patients with heart failure : results from the International Congestive Heart Failure (INTER-CHF) prospective cohort study. 2017; 665-72. |
| [42] | Callender T, Woodward M, Roth G, Farzadfar F, Lemarie JC, Gicquel S, et al. Heart failure care in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2015; 11(8). |
| [43] | Miró Ò, García Sarasola A, Fuenzalida C, Calderón S, Jacob J, Aguirre A, et al. Departments involved during the first episode of acute heart failure and subsequent emergency department revisits and rehospitalisations: an outlook through the NOVICA cohort. Eur J Heart Fail. 2019; 21(10): 1231-44. |
| [44] | Butt JH, Fosbøl EL, Gerds TA, Andersson C, McMurray JJV, Petrie MC, et al. Readmission and death in patients admitted with new-onset versus worsening of chronic heart failure: insights from a nationwide cohort. Eur J Heart Fail. 2020; 22(10): 1777-85. |
| [45] | CSA ECSA. Ethiopian 2022 Project Population Census. 2022; (July). |
| [46] | Chen X. Chinese clinical practice guideline for acute kidney injury. Natl Med J China. 2023; 103(42): 3332-66. |
| [47] | Is H, Use A. Preventing Cancer by Reducing Excessive Alcohol Use How Is Alcohol Use Defined ? What Is Considered One Drink ? What Are the Guidelines for Alcohol Use ?: 23-4. |
| [48] | Keller K. National Center for Health Statistics. Encycl Obes. 2014; 23-4. |
| [49] | Survey H. Ethiopia. 2016. |
| [50] | Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022; |
| [51] | Demisse L, Alemayehu B, Addissie A, Azazh A, Gary R. Knowledge, attitudes and beliefs about acute coronary syndrome among patients diagnosed with acute coronary syndrome, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2022; 22(1): 1-9. Available from: |
APA Style
André, M. C., Emmanuelle, D. G., Honorine, R. E. S. (2025). Seroprevalence of IgG Antibodies Against Herpes Simplex Virus 1 and 2 in Children Born HIV Positive at the Yaounde University Teaching Hospital. International Journal of Biomedical Engineering and Clinical Science, 11(3), 40-46. https://doi.org/10.11648/j.ijbecs.20251103.11
ACS Style
André, M. C.; Emmanuelle, D. G.; Honorine, R. E. S. Seroprevalence of IgG Antibodies Against Herpes Simplex Virus 1 and 2 in Children Born HIV Positive at the Yaounde University Teaching Hospital. Int. J. Biomed. Eng. Clin. Sci. 2025, 11(3), 40-46. doi: 10.11648/j.ijbecs.20251103.11
@article{10.11648/j.ijbecs.20251103.11,
author = {Mbongue-Mikangue Chris André and Dikabo-Mikangué Grace Emmanuelle and Riwom Essama Sara Honorine},
title = {Seroprevalence of IgG Antibodies Against Herpes Simplex Virus 1 and 2 in Children Born HIV Positive at the Yaounde University Teaching Hospital
},
journal = {International Journal of Biomedical Engineering and Clinical Science},
volume = {11},
number = {3},
pages = {40-46},
doi = {10.11648/j.ijbecs.20251103.11},
url = {https://doi.org/10.11648/j.ijbecs.20251103.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbecs.20251103.11},
abstract = {Background: Infection with the Human Immunodeficiency Virus (HIV) is responsible for the terminal stage of Acquired Immunodeficiency Syndrome (AIDS), which was a latent infection until the introduction of antiretroviral treatment. The progression to chronicity of this infection leads to chronic inflammation that facilitates the occurrence of opportunistic infections such as herpes simplex virus types 1 and 2 (Herpes Simplex Virus-1 (HSV-1) and Herpes Simplex Virus-2 (HSV-2)). The lack of data on these viruses has led to the present study. Objective: aimed to determine the seroprevalence of IgG antibodies against herpes simplex virus types 1 and 2 in children born HIV-positive to HIV-positive mothers with an undetectable viral load and receiving antiretroviral treatment at the Yaoundé University Teaching Hospital (YUTH). Method: The study was cross-sectional conducted after 12 months of follow up. After administering a questionnaire, a blood sample was obtained from each participant in an EDTA tube and analyzed using rapid diagnostic tests for the detection of specific IgM/IgG antibodies. Statistical analysis was performed using Microsoft Excel 2019 and SPSS version 25. A P-value Result: Among the 74 participants, 51 were female, resulting in a sex ratio of 0.45. In the population of children born HIV-positive, the seroprevalence was 93.24% (n=69) for IgG anti-HSV-1, 93.24% (n=69) for IgG anti-HSV-2, and 93.24% (n=69) for IgG anti-HSV-1/-2. The seroprevalence of IgM anti-HSV was found to be zero; however, the prevalence of IgG anti-HSV was 93.24%. The seroprevalence of HSV-1/-2 was associated with the age of the participants. Conclusion: It can be concluded that the herpes simplex virus circulates in Cameroon, with a high presence of anti-HSV-1/-2 antibodies in the population born HIV-positive to HIV-positive mothers. It becomes important to implement systematic diagnostic measures for children born HIV-positive to HIV-positive mothers, and its transmission is associated with various risk factors.
},
year = {2025}
}
TY - JOUR T1 - Seroprevalence of IgG Antibodies Against Herpes Simplex Virus 1 and 2 in Children Born HIV Positive at the Yaounde University Teaching Hospital AU - Mbongue-Mikangue Chris André AU - Dikabo-Mikangué Grace Emmanuelle AU - Riwom Essama Sara Honorine Y1 - 2025/09/09 PY - 2025 N1 - https://doi.org/10.11648/j.ijbecs.20251103.11 DO - 10.11648/j.ijbecs.20251103.11 T2 - International Journal of Biomedical Engineering and Clinical Science JF - International Journal of Biomedical Engineering and Clinical Science JO - International Journal of Biomedical Engineering and Clinical Science SP - 40 EP - 46 PB - Science Publishing Group SN - 2472-1301 UR - https://doi.org/10.11648/j.ijbecs.20251103.11 AB - Background: Infection with the Human Immunodeficiency Virus (HIV) is responsible for the terminal stage of Acquired Immunodeficiency Syndrome (AIDS), which was a latent infection until the introduction of antiretroviral treatment. The progression to chronicity of this infection leads to chronic inflammation that facilitates the occurrence of opportunistic infections such as herpes simplex virus types 1 and 2 (Herpes Simplex Virus-1 (HSV-1) and Herpes Simplex Virus-2 (HSV-2)). The lack of data on these viruses has led to the present study. Objective: aimed to determine the seroprevalence of IgG antibodies against herpes simplex virus types 1 and 2 in children born HIV-positive to HIV-positive mothers with an undetectable viral load and receiving antiretroviral treatment at the Yaoundé University Teaching Hospital (YUTH). Method: The study was cross-sectional conducted after 12 months of follow up. After administering a questionnaire, a blood sample was obtained from each participant in an EDTA tube and analyzed using rapid diagnostic tests for the detection of specific IgM/IgG antibodies. Statistical analysis was performed using Microsoft Excel 2019 and SPSS version 25. A P-value Result: Among the 74 participants, 51 were female, resulting in a sex ratio of 0.45. In the population of children born HIV-positive, the seroprevalence was 93.24% (n=69) for IgG anti-HSV-1, 93.24% (n=69) for IgG anti-HSV-2, and 93.24% (n=69) for IgG anti-HSV-1/-2. The seroprevalence of IgM anti-HSV was found to be zero; however, the prevalence of IgG anti-HSV was 93.24%. The seroprevalence of HSV-1/-2 was associated with the age of the participants. Conclusion: It can be concluded that the herpes simplex virus circulates in Cameroon, with a high presence of anti-HSV-1/-2 antibodies in the population born HIV-positive to HIV-positive mothers. It becomes important to implement systematic diagnostic measures for children born HIV-positive to HIV-positive mothers, and its transmission is associated with various risk factors. VL - 11 IS - 3 ER -
Department of Microbiology, The University of Yaounde I, Yaounde, Cameroon
Department of Didactics, The University of Yaounde I, Yaounde, Cameroon
Department of Microbiology, The University of Yaounde I, Yaounde, Cameroon